PARAMORPHIC AND DYSMORPHIC CHANGES OF THE THORAX IN CHILDREN AT THE AGE BETWEEN 11 AND 14
Zdenko Kosinac, Jelena Bižaca
Department of Physical Education, Faculty of Natural Sciences Mathematics and Education, University of Split, Teslina 12, 21000 Split, Croatia
THE PROBLEM
The complex organic functional transformation with a developing person does not proceed regulary and equally in all the parts of an organism, but they proceed rhythmically, according to the course which is influenced by the hereditary-constitutional, auxological, endocrinological and environmental factors. In this long period of morphologic-motoric, physiological and psychical transformations, bigger or smaller deviations can occur, which temporarily or permanently change the orthostatic posture. The paramorphic and dysmorphic changes of the thorax do not occur so often, but as they can cause many psychosomatic and functional problems, they deserve a bigger medical-therapeutic attention than has been paid so far.
MATERIALS AND METHODS
The research has been done on a specimen of 320 testees between the age of 11 and 14, which were divided into two subsamples according to gender. The testees underwent a somatic examination according to the instructions given by Lekszas (1981) and Pećina (1987) about the check-up of the motion system. A group of 19 relevant anthropometric and somatic indicators have been applied, which show the paramorphic and dysmorphic changes of the thorax. These are the indicators: body height (BH), body weight (BW), biacromial range (BIAKR), the depth of the thorax (DTHO), the average thorax volume (AVTHC), the width of the thorax (WDTH), the minimal waist volume (MINWV), subscapular skin fold (SCSF), axillar skin fold (AXSF), the shoulder symmetry (SHSYM), the shoulder-blade symmetry (SHBSYM), the chest muscles symmetry (CMSYM), the symmetry of Lorenz’s angle (SYMLA), pectum carrinatum (PECCAR), pectum excavatum (PECEXC), epigastric angle (EPASYM), the thorax kyphosis (THOKYF), the thorax scoliosis (THOSCO), the elasticity of ribs (ELASRIB).
The information about the differences among the adolescent groups according to gender have been determined by the complete discriminative procedures. These are: the testing on the importance of the differences between the central variable parameters with the help of the analysis of variance and the canonical discriminative analysis.
RESULTS AND DISCUSSION
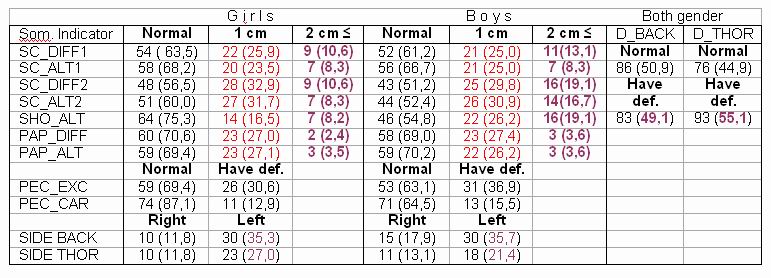
On the basis of statistic parameters, the frequencies and percentages for each group and every level of education separately, one can state that the paramorphic changes of the thorax posture relatively often occur in younger adolescents. In general the asymmetry of the shoulder-blades posture, Lorenz’s angle and the front part of the thorax (epigastric triangle and chest muscles) occurs more often with boys and girls of the seventh and eighth grade. Concerning the gender it is evident that boys have the bigger percentage of different forms of paramorphic changes of the thorax. That is due to the uneven dynamics of the changes in a particular segment of the thorax, the length of the thorax grows faster than its transversal and front back diameters, as well as the fact that the thorax is still not completely formed at the age of 14. As it grows, the process of morphologic shaping continues. The hereditary- constitutional influence and the influences of the so-called environmental factors ( poor posture when sitting, inadequate burdening and tiredness) in the sensitive period of puberty is not to be ignored. By inspecting the tables 1 and 2 it is obvious that boys more often have the asymmetry of the posture of some thorax structures. This conclusion is current in boys and girls of the eighth grade, who have evidently bigger percentage of the paramorphic thorax changes. The posture of shoulder-blades is the most common dysfunction of the shoulder area (35-50% in girls, 45-62% in boys) and it is often connected with the above mentioned factors, which results with differences in deviation, among which most often occur: the so-called alated shoulder-blades (scapula alatae – often accompanied by the bent back), uneven shoulder-blades – not in the same level (as a result of scoliosis), lowered shoulders “as a bottle neck” (often comes along with bad posture when standing) and a shoulderless silhouette or “a happy neck” (the result of the insufficient front chest muscles) are the most often dysfunctions of the thorax posture (35-50% in girls, 45-62% in boys). The presence of the carinal thorax (pectus carinatum) in younger adolescents is about 16%, whilst the same percentage is smaller in girls and is about 7.5%. According to the gender we have established with girls: 1st degree (5.6%), 2nd degree (1.9%); in boys: 1st degree (10%), 2nd degree (6.3%). In the both specimen not a single case of the 3rd degree has been established, which was to expect, since the deformity progresses with the growth and in a relatively short period of time the thorax bone protrudes out for several centimetres. The cause of this deformity is connected with rickets and as a family anomaly it often comes together with other congenital anomalies and diseases (a heart condition, asthma, etc). The funnel-like thorax (pectus excavatum) is a rare dysmorphic form of the thorax (around 11% in boys, around 6% in girls). This change of the thorax form still deserves more medical – therapeutic and kinesiological attention (because it can have multiple negative consequences). The posture appearance is completed by the increased presence of the bent spine in sagittal plain backwards. The physiological sagittal bend of the thorax spine is in much bigger percentage present in boys. During the fast growth in the period of adolescence the spine is exposed to many mechanic impacts with possible anthropologic, functional and structural changes and disorders. The special vulnerability is present with tall, gracile and insufficiently nourished boys and girls, who are exposed to bigger burdenings at a very early age. In the early childhood they are usually manifested as a form of the poor posture. By reaching the puberty the kyphoscolioticaly bent spine becomes easy to diagnose and less likely to be reduced, and many of them show progressive fixation which gets stabilised after they stop growing. Concerning the frequency, the characteristics of the period of growth and development, the influence of mechanical factors and stresses, the localisation and the characteristic changes, as well as the possibilities of therapeutic results, juvenile kyphoses deserve a special attention of kinesiologists and biomechanics. The latest researches show that the pathologic processes on the spine in adults develop exactly on the place of the biggest physiological distortion of the thorax spine (Tribastone, 1994). On the contrary, the juvenile age is characterised by the low localisation of the thorax kyphosis (Schmorl, Guntz, Ruskowski etc.). These cognitions put under suspicion those theories, which consider the overburdening of the spine as the prime cause of kyphosis. The thoughts of Dürring (1972) are worth making current once again because of some practical reasons. He finds it necessary to search for the conceived signs of a part of the thorax or thoracolumbial spine – which are initial signs of the juvenile kyphosis. “In this way we will be able to single those individuals out of a large group of muscle weaklings with the obviouse poor posture, on whom the kyphosis or Scheuerman’s disease may develop.” The right way leads from the early diagnosis to getting involved in certain therapeutic procedures and chosen sport activities with a strong antiparamorphic effect. If not so, in the next phase (after the age of 14) a definite clinical diagnosis is found with the fixed dorsal kyphosis, and the prospects for the effective therapy are small. The vectors of the arithmetic means of the groups defined by the system of 9 anthropometric variables and ten paramorphic and dysmorphic chest changes indicators differ very much from each other. The results of Wilkes’ test and Barttlet’s tests in the table 1 show that. The discriminative variant on which the groups differ with the square coefficient .48, which equals the coefficient of the canonical discrimination of .57, and in this way 57% of the group variant is being taken. Since the groups differed very much in the anthropometric space and the space of some paramorphic and dysmorphic indicators of the thorax changes, it was justified to analyse the differences among the groups in every variable separately. The results of the variant analysis (Table 3) show that the groups of testees defined by gender differ very much in variables for estimation of the thorax symmetry, Lorenz’s triangle symmetry, epigastric angle, thorax kyphosis, shoulder-blades symmetry, axillar skin fold, carinal thorax on the level P= .01, and the funnel-shaped thorax, subscapular skin fold, thorax width, biacromial range, thorax depth and the minimal waist volume. On the level p= .05. The first and only discriminative variable is defined positive by variables of height, axillar skin wrinkle, subscapular skin wrinkle, whilst on the negative pole it is defined by the variables the depth of the thorax, the minimal waist volume I., biacromial range, and the asymmetry of the chest muscles, the funnel-like thorax and the asymmetry of Lorenz,s triangle. But the most important key how to separate the testees has the variable the depth of the thorax, the minimal waist volume I. And biacrominal range. Concerning the arithmetic means and the direction of centroids (Table 3) it can be expected that boys have bigger diameters of the thorax and waist, but at the same time some paramorphic and dysmorphic thorax changes are more likely to be present. The differences in height are expected and they match the results of some previous researches (Girova, 1977, Kosinac 1997). The mentioned researches show that female children with a scoliotic spine grow faster in the prepuberty phase. During puberty these differences decrease little by little, and at the age of 15 the differences in height almost disappear. Lončar-Dušek and their co-operators (1998) consider that the girls with whom the scoliotic distortion of the spine was diagnosed in puberty, grow faster than boys in adolescence. If the fast growth, which is under nervous hormonal influence, is connected with the time and the increase of the spine distortion, it can be expected that the children who grow fast make a group of risky children exposed to the scoliotic spine. If we take into consideration the coming period of the fast growth in adolescence, the further deterioration of the initial paramorphic changes can be predicted, as well as the possible transformation in the inevitable dysmorphism, with reduced therapeutic expectations.
CONCLUSION
The results of canonical discriminative analysis show the very important function (Table 3) which specifically separates the groups of adolescents acoording to gender, when the analysed anthropomertic variables and indicators of the paramorphic and dysmorphic thorax changes are taken into consideration. Bigger thorax and waist diameters have been established in boys, but at the same time the paramorphic and dysmorphic changes of the thorax and the surrounding structures are more often present. Girls are characterised by bigger amounts of subcutaneous fat tissue and bigger height.
The results of canonical discriminative analysis show the very important function (Table 3) which specifically separates the groups of adolescents acoording to gender, when the analysed anthropomertic variables and indicators of the paramorphic and dysmorphic thorax changes are taken into consideration. Bigger thorax and waist diameters have been established in boys, but at the same time the paramorphic and dysmorphic changes of the thorax and the surrounding structures are more often present. Girls are characterised by bigger amounts of subcutaneous fat tissue and bigger height.
BIBLIOGRAPHY
1. Antropova, M.V., Koljcova,M.M.(1983): Psihofizička zrelost dece.Beograd:Zavod za
udžbenike i nastavna sredstva, p.139:174
2. Gyrova, N.I.(1977): Vozrastanja morfologija trudnoj kletki čeloveko, Moskva, p.215
3. Kosinac, Z. (1997): Kinineziologija, 29, 2:26:33
4. Lekszas, G. (1981): heilsport in der Orthopadie. Ferdinand Enke Verlag, Stuttgart
5. Tribastone, R. (1994): Compedio Ginastica Corretiva. Societa Stampa Sportiva, Roma.
Kosinac Z and J Bižaca (2002). Paramorphic and dismorphic changes of the thorax in children at the age between 11 and 14. Proceedings book of 3. Kinesiology – New perspectives. Opatija. p 537-540.